How to Write SOAP Notes: Template, Examples, Audit Checklist
SOAP notes are a structured way to document a patient encounter: Subjective, Objective, Assessment, and Plan. A good SOAP note does more than fill four headings. It separates the patient's story from measured findings, explains the clinician's reasoning, and gives the next provider a plan that can be followed without guessing.
This guide is for clinicians, students, care coordinators, and operations teams who need a practical SOAP note template and a safer review routine. It is not medical, legal, billing, or compliance advice. Always follow your EHR policy, payer rules, state or country requirements, and your organization's privacy and documentation standards before signing a record.
SOAP Notes at a Glance
| Section | Main question | Include | Avoid |
|---|---|---|---|
| Subjective | What did the patient report? | Chief complaint, HPI, relevant history, patient quotes, pertinent negatives | Diagnosis, interpretation, copied symptoms that were not verified today |
| Objective | What can be observed or measured? | Vitals, exam findings, labs, imaging, observed behavior, telehealth limits | Clinical conclusions, speculation, unsupported severity language |
| Assessment | What does the information mean? | Working diagnosis, differential, risk, status vs. baseline, reasoning | A plan without rationale, vague labels, unexplained uncertainty |
| Plan | What happens next? | Orders, medications, therapy, education, follow-up, safety instructions, monitoring | "PRN" or "continue" without detail, tasks not tied to a problem |
Use SOAP when clarity and traceability matter: initial evaluations, complex cases, multi-provider handoffs, therapy progress notes, medication management, and encounters that may later be reviewed for medical necessity. For patient-facing absence documentation, see our doctor's note template. For a related mental-health format, compare DAP notes examples.
Step 1: Define the SOAP Framework Before You Write
The biggest SOAP note mistake is treating the format as four generic boxes. Each section has a job.
- Subjective captures the patient's experience in their own words.
- Objective records facts that can be observed, measured, or reviewed.
- Assessment explains the clinician's interpretation of those facts.
- Plan documents the next clinical, educational, and follow-up actions.
Before writing, decide what problem the note is documenting and what another clinician or auditor would need to understand the encounter. That single framing step prevents note bloat. It also reduces copy-forward drift, because every sentence must earn its place in today's record.
Quick standard: if a sentence does not support today's complaint, risk, diagnosis, or plan, delete it or move it to the correct section.
Step 2: Write the Subjective Section With OLDCARTS and Pertinent Negatives
The Subjective section should tell a focused patient story. Start with the chief complaint, then structure the history of present illness with a repeatable framework such as OLDCARTS: onset, location, duration, character, aggravating/alleviating factors, radiation, timing, and severity.
| Better subjective note | Weak subjective note |
|---|---|
| CC: "left-sided chest pressure." HPI: 54-year-old patient reports sudden heavy chest pressure starting 2 hours ago while gardening, radiating to jaw, worse with exertion, improved with rest; denies fever, cough, or prior similar episode. | Chest pain for a while. |
| CC: "stomach hurts after meals." HPI: 34-year-old patient reports 2 weeks of burning epigastric pain after meals, worse with spicy foods, partially relieved by antacids; denies vomiting, melena, or unintentional weight loss. | Stomach pain. Not sure when it started. |
Good subjective documentation includes what the patient says and what the patient denies when those negatives affect the differential. Do not diagnose in this section. Save interpretation for Assessment.
Subjective checklist
- Quote the chief complaint when useful.
- Include relevant history, medications, allergies, and review of systems.
- Add 1-2 pertinent negatives that change risk or differential thinking.
- Flag urgent symptoms clearly: syncope, severe pain, neurologic changes, shortness of breath, suicidal ideation, or other specialty-specific red flags.
- Keep the story short enough that the next clinician can scan it quickly.
Step 3: Keep Objective Findings Verifiable
Objective findings should be observable, measurable, or available in the record at the time of documentation. Examples include vital signs, exam findings, lab and imaging results, clinician-observed behavior, and telehealth exam limitations.
If you use a normal physical exam template, only keep the normal findings you actually assessed today. Auto-populated normals can create audit and patient-safety risk when they contradict the visit type or the patient's complaint.
| Objective category | Concise example |
|---|---|
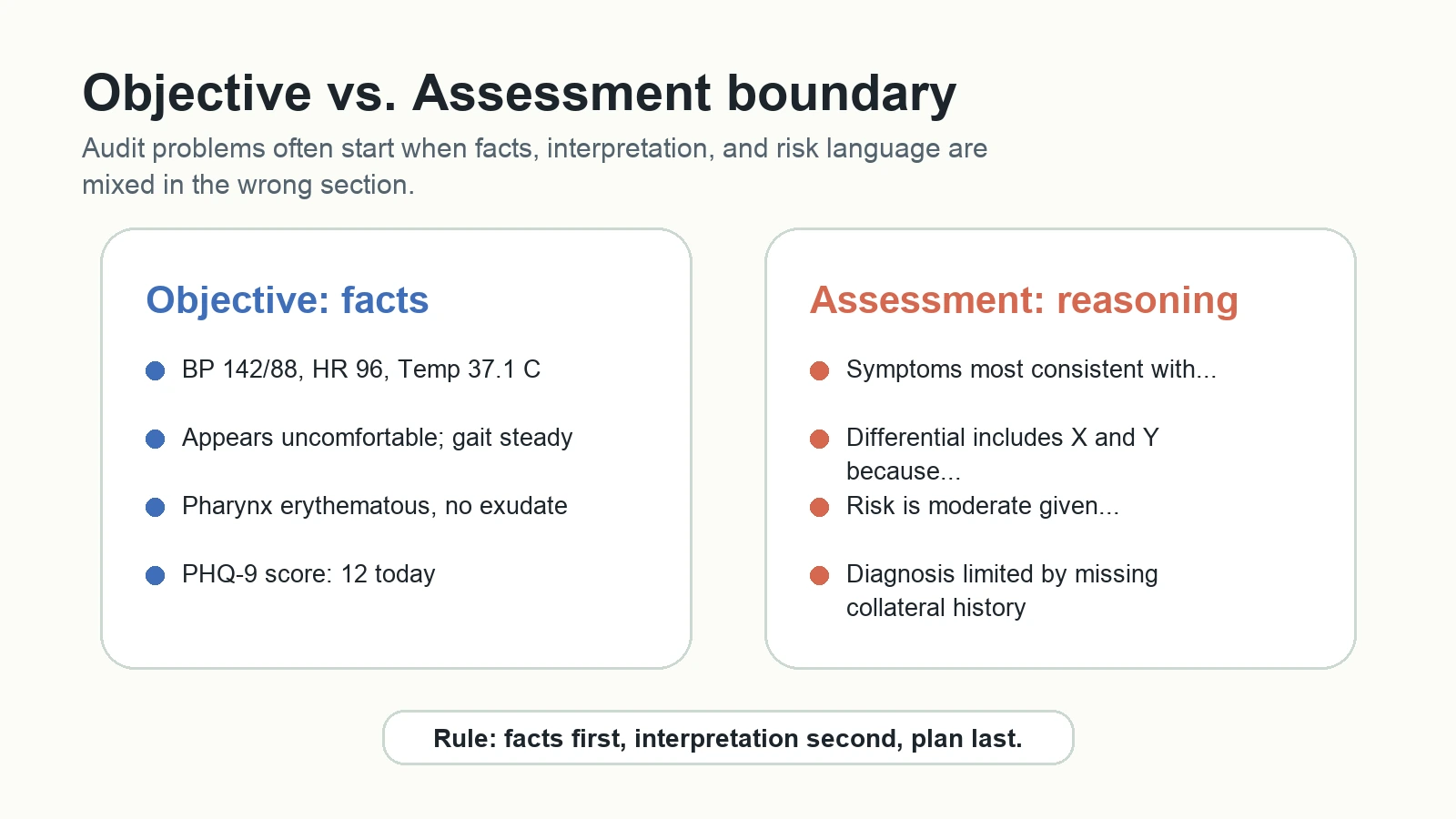
| Vitals | BP 142/88, HR 96, RR 18, Temp 37.1 C, SpO2 98% RA |
| General | Alert, oriented, appears uncomfortable but not in acute distress |
| HEENT | Oropharynx erythematous, no tonsillar exudate, mucous membranes moist |
| Mental status | Well-groomed, cooperative, speech normal rate/volume, mood "anxious," affect congruent, thought process linear |
| Telehealth limitation | Video visit; abdominal palpation not performed. Patient instructed on red flags and escalation. |
Objective checklist
- Include only data available during the encounter.
- Separate observed behavior from interpretation.
- Use standard abbreviations only when your organization approves them.
- Describe abnormal findings with location, quality, and severity.
- State limitations, especially for telehealth or incomplete exams.
Step 4: Make the Assessment Show Clinical Reasoning
Assessment is where SOAP notes become defensible. It should connect the Subjective and Objective evidence to a working diagnosis, differential, and risk level. Avoid unsupported labels such as "likely anxiety" without explaining why the documented facts point there.
A practical assessment structure:
- State the primary problem or diagnosis.
- Give a one-sentence rationale using subjective and objective evidence.
- List 1-3 differentials when clinically appropriate.
- Explain why each alternative is more or less likely.
- State risk, severity, or limitations in available data.
Example:
Symptoms most consistent with acute viral pharyngitis given sore throat, erythematous oropharynx, absence of tonsillar exudate, and afebrile vitals. Streptococcal pharyngitis remains in differential due to throat pain; rapid test ordered. No signs of airway compromise today.
For behavioral health notes, the same rule applies: tie every interpretation to documented symptoms, observed behavior, assessment tools, or risk evaluation. If data is incomplete, say so plainly rather than overstating certainty.
Step 5: Write a Plan Another Clinician Can Follow
The Plan section should be actionable. A strong plan links every intervention to the assessed problem and includes enough detail for a covering clinician to understand what was ordered, why, and when to reassess. The examples below are documentation examples, not treatment protocols.
| Plan item | Strong documentation example | Weak documentation example |
|---|---|---|
| Medication | Record the ordered medication name, dose, route, frequency, start date, counseling, and monitoring plan according to the signed clinical order. | Start medication. |
| Monitoring | Track PHQ-9 at each visit for 4 weeks; patient will call sooner for worsening mood or suicidal thoughts. | Monitor symptoms. |
| Education | Discussed hydration, expected course, return precautions for fever, shortness of breath, or worsening pain. | Patient educated. |
| Referral | Refer to ENT if hoarseness persists beyond 4 weeks or red flags develop. | Refer if needed. |
SMART goals can help, but do not force every medical plan into corporate wording. The useful standard is traceability: each plan item should connect back to a problem and include timing, ownership, or escalation criteria.
Plan checklist
- Orders, medications, referrals, and therapies are specific.
- Patient education and shared decision-making are documented when relevant.
- Follow-up interval is clear.
- Safety-net instructions are explicit.
- Progress notes state what changed since the last visit instead of copying the same plan forward.
Step 6: Use EHR Templates Without Creating Stale Notes
Templates save time only when they prompt current thinking. They become dangerous when they insert old findings, outdated problem lists, or generic normal exams that were not checked today.
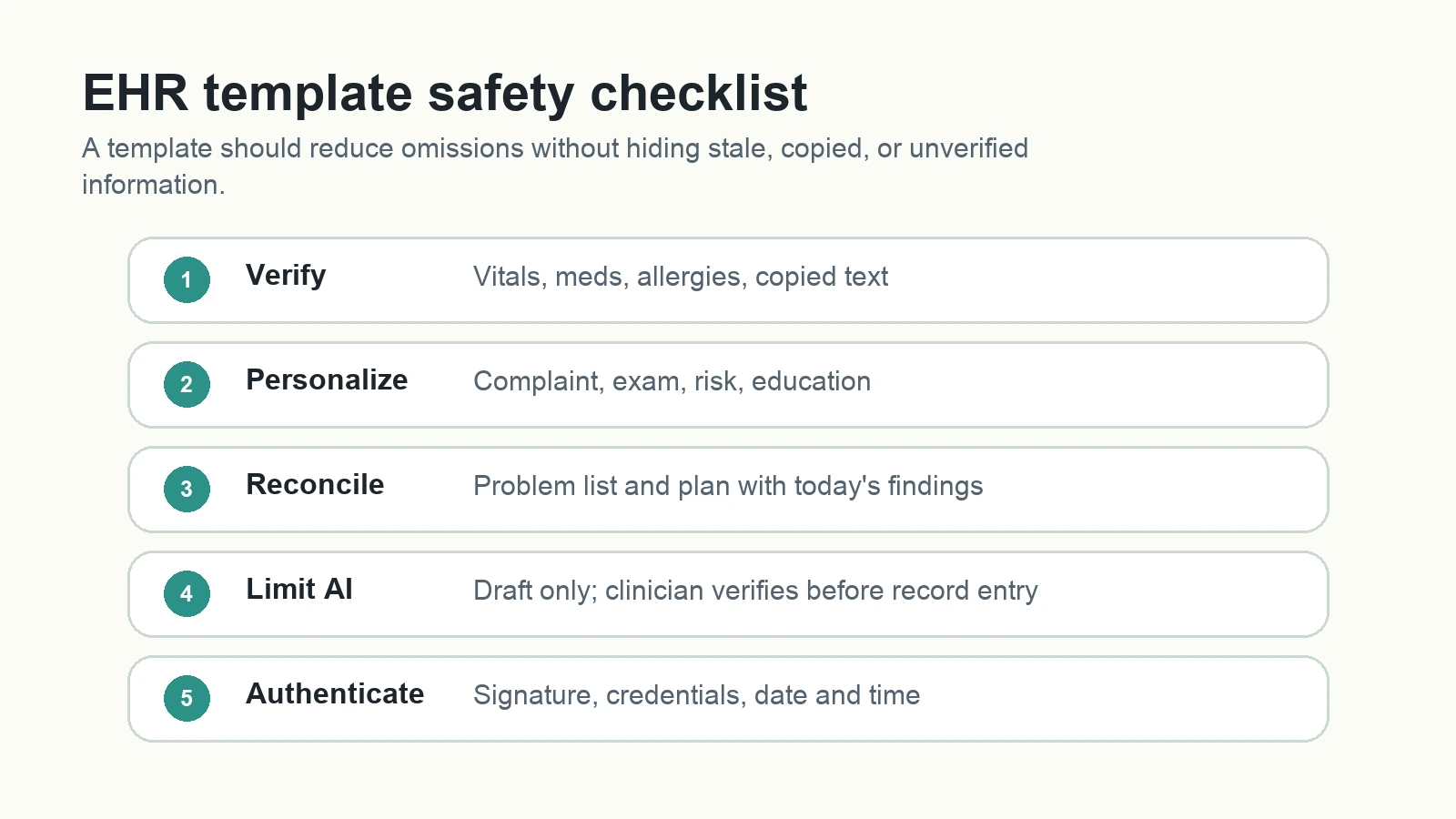
Build a SOAP note template around prompts, not long canned paragraphs:
- Subjective: chief complaint, HPI framework, relevant history, pertinent negatives.
- Objective: vitals, focused exam, diagnostics, telehealth limits.
- Assessment: problem, rationale, differential, risk, uncertainty.
- Plan: intervention, patient education, monitoring, follow-up, escalation.
- Final review: copy-forward check, approved abbreviations, signature, time stamp.
Structured fields are useful for vitals, medications, allergies, screening scores, and discrete yes/no findings. Free text is better for patient story, clinical reasoning, and unusual context. Use both intentionally.
Step 7: Set Clear Rules for AI-Assisted SOAP Drafting
AI can help organize notes, summarize dictated details, or turn rough observations into a draft. It cannot replace clinician judgment or organizational privacy review. Do not paste protected health information into tools your organization has not approved.
Minimum AI review rules:
- Verify every fact against the encounter and source record.
- Remove invented symptoms, findings, diagnoses, or plan items.
- Confirm the draft separates Subjective, Objective, Assessment, and Plan correctly.
- Check privacy policy, retention settings, and approved vendor status before any PHI workflow.
- Sign only after a licensed clinician has reviewed the final note.
AI can draft structure. Clinicians must verify content.
Step 8: Correct, Amend, and Authenticate Notes Transparently
If you find an error after signing a note, do not silently overwrite the record. Follow your EHR and compliance policy for corrections, addenda, late entries, and time stamps. The general principle is traceability: a reviewer should be able to see what changed, when, why, and by whom.
Use a consistent correction routine:
- Label the change as an addendum, correction, or late entry.
- Include the current date and time.
- State the original error and the corrected information.
- Sign with name and credentials.
- Notify the care team if the correction changes clinical management.
For abbreviations, maintain a local approved list and review it regularly. The Joint Commission's Do Not Use list is a useful safety reference for avoiding ambiguous shortcuts such as "U," "IU," trailing zeros, or missing leading zeros.
Step 9: Standardize SOAP Notes in a Shared Workspace
Teams usually lose consistency because templates, approved abbreviations, care pathways, and audit feedback live in different places. A shared workspace solves that by keeping the current SOAP note template, review checklist, examples, and update history together.
In AFFiNE's infinite whiteboard, a team can map complex care pathways visually, then keep the detailed SOAP template in page mode. In AFFiNE, you can maintain:
- A master SOAP note template by specialty or visit type.
- Approved abbreviation and do-not-use lists.
- Example notes for onboarding and student training.
- Progress tables for recurring visits.
- A revision log that records template owner, last review date, and source updates.
This matters for E-E-A-T as well as clinical operations. A visible review process, clear source list, and dated update log make the page more trustworthy for readers and easier for teams to maintain.
SOAP Note Template You Can Adapt
S: Chief complaint:
HPI:
Relevant history:
Medications/allergies:
Pertinent positives:
Pertinent negatives:
O: Vitals:
Focused exam:
Diagnostics available today:
Observed behavior:
Visit limitations:
A: Primary assessment:
Rationale:
Differential:
Risk/severity:
Data limitations:
P: Orders/interventions:
Medications or therapy:
Patient education:
Monitoring:
Follow-up:
Return precautions:
Signature/date/time:
Final SOAP Note Audit Checklist
Before signing, review the note against these questions:
- Does the title or visit type match the actual encounter?
- Are patient quotes and symptoms current for this visit?
- Are objective findings measurable, observed, or available now?
- Does the assessment explain why the plan is medically necessary?
- Does every plan item trace to a documented problem?
- Did you remove stale copy-forward text?
- Are abbreviations approved by your organization?
- Is any AI-generated language fully verified?
- Are addenda, late entries, signatures, and time stamps handled according to policy?
Frequently Asked Questions About SOAP Notes
What does SOAP stand for in medical documentation?
SOAP stands for Subjective, Objective, Assessment, and Plan. The structure helps clinicians separate the patient's report, measurable findings, clinical reasoning, and next steps.
Who uses SOAP notes?
SOAP notes are used by physicians, nurses, therapists, behavioral health clinicians, care coordinators, and students. The exact content depends on specialty, setting, payer requirements, and organizational policy.
Can ChatGPT write SOAP notes?
ChatGPT and other AI tools can help draft or organize SOAP-style text, but clinicians must verify every fact, diagnosis, and plan item before the note enters the medical record. Do not use unapproved AI tools with protected health information.
How do you make SOAP notes audit-friendly?
Keep each section distinct, tie the Assessment to documented evidence, make the Plan measurable, remove stale copied text, and include clear signatures, dates, and follow-up instructions.
What is the most common SOAP note mistake?
The most common mistake is mixing interpretation into Objective or writing a Plan that does not connect to the Assessment. A second common mistake is copying old template text without verifying that it is true for the current encounter.
Sources and Review Notes
This article was refreshed as a documentation workflow guide, not a clinical treatment protocol. It was reviewed for clear scope, source naming, privacy boundaries, image alt text, and current AFFiNE editorial standards. Practical references include the Joint Commission abbreviation safety guidance, commonly used patient-history frameworks such as OLDCARTS, and AFFiNE's public editorial policy.